한국 여성의 비만과 체형인식왜곡에 따른 유방암 검진율 차이
Differences in Breast Cancer Screening Rates according to Obesity and Weight Perception among Korean Women
Article information
Abstract
Purpose: This study was performed to elucidate whether the obesity or body image is a barrier to breast screening compliance in Korean women. Methods: We included 54,017 women aged between 35 to 70 years from the Korea Community Health Survey (KCHS) 2014 dataset. To identify whether a mutual relationship exists between weight perceptions and breast cancer screening rates, the participants were divided into three groups according to the level of concordance between Body Mass Index (BMI) and a subjective body image. Descriptive analyses, a chi-square test, and multivariate logistic regression analyses were performed. Results: After covariate adjustment, the screening rate of the overweight group was 1.09 times higher than the normal weight group (odds ratio [OR], 1.09; confidence interval [CI], 0.00-0.16; p=.038) and the severe obesity group was 1.20 times lower (OR, 0.83; CI, -0.36-0.00; p=.047). Weight misperception also had a significant influence on breast cancer screening. Especially, The overweight distortion group was less likely to undergo breast cancer screening (OR, 0.93; CI, -0.15-0.00; p=.037). Conclusion: Obesity and weight misperceptions are associated with lower compliance with breast cancer screening guidelines.
서 론
한국 여성의 연령 표준화 암 발생률의 추이를 보면, 다른 암종들 은 감소하는 경향을 보이나 유방암은 2005년부터 2014년까지 연평 균 4.5%씩 꾸준히 증가하고 있어 유방암 발생 예방을 위한 노력이 더욱 촉구되는 상황이다[1]. 특히 비만은 유방암 발생의 대표적인 위험인자이다. 세계보건기구의 국제암연구협회는 비만과 활동량 감소가 유방암의 발생 위험을 높인다고 경고하였다[2]. 이는 지방세 포에서 분비되는 에스트로겐이 세포 분화를 촉진해 세포 분화 과 정에서 이형성 세포가 생길 확률이 증가하여 악성 종양의 발생 확 률이 증가하기 때문으로 추측한다[3-5].
따라서 유방암 발병을 예방하기 위해서는 건강행동을 통한 사 전 예방이 가장 효과적이나 현실적인 이유로 국가에서는 2차 예방 수단인 암 조기 검진을 장려하고 있다. 이에 유방암 발병 위험률이 높은 비만 여성에게 있어 유방암 검진이 중요하지만, 이들의 암 검 진율은 일반여성보다 낮다는 보고가 있다[6,7]. 이를 두고, 비만이 예방적 건강행동과 의료이용에 보이지 않는 걸림돌이 된다는 주장 이 있다. 비만 자체가 문제가 되는 것이 아니라 사회 전반에 퍼지게 된 비만 집단에 대한 부정적 인식이 예방적 건강행동과 의료이용에 걸림돌이 된다는 것이다[8,9]. ‘뚱뚱한 몸’은 게으르며 의지가 약하고 비지성적이며 자기 규율이 부족한 사람의 몸이라는 편견이 있다[8]. 따라서 비만은 충분히 극복할 수 있는 개인의 문제로 치부되어 비 만 집단은 자기관리에 실패한 의지력이 약한 집단으로 여겨지기 쉽 다. 이로 인해 비만 집단조차 이러한 편견을 내면화하여 부정적인 신체 이미지를 갖게 되며, 비만은 본인의 실패로 여기게 된다[10]. Amy 와 Caren [11]의 연구에 따르면, 498명의 연구대상자 중 68%는 자신 이 비만하다는 이유로 의료이용을 주저한 경험이 있다고 응답하였 으며 그 이유로 치료의 불신 및 의료인의 부정적인 태도와 의사소 통 과정에서 느끼는 수치심 등을 주요 원인으로 꼽았다.
Ridolfi와 Crowther [12]는 선행연구와 관련 이론들을 종합해 비만 과 같은 부정적 신체 이미지가 신체 노출 방식의 암 검진에 영향을 끼 치는 기전을 모델로 제시하였다. 특히 부정적 신체 이미지는 여성의 신체에 대한 부끄러움(body shame)이나 신체 회피(body avoidance)로 이어지고 자아 존중감, 사회적 규범, 건강에 대한 불안, 나이, 위험 지각 등의 조절 효과를 통해 신체 노출 방식의 암 검진에 부정적 영 향을 끼친다[12]. 이는 비만에 대한 부정적인 인식이 암 검진과 같은 의료이용 혹은 예방적 건강행동에 장애물로 작용할 수 있음을 시 사한다.
일반적으로 유방암 검진의 영향요인을 연구한 연구들은 인구 사 회학적 특성이나 건강행동에 관한 심리학 모형을 이용하여 검진 수 검 의도를 설명하는 연구가 다수이다[13]. 최근에는 건강행동들이 서로 연관(clustering)되어 있어[14] 다른 건강행동을 실천하는 사람 들이 건강검진 역시 잘 이행한다는 보고도 있다[15,16].
그러나 의료현장에서 비만 집단의 고립이나 비만에 대한 부정적 인식으로 인한 의료이용 저하 등을 뒷받침할 국내 연구는, 비만과 유 방암, 자궁경부암의 검진에 있어 음의 상관관계를 입증한 연구[17] 한 편이 유일하다. 또한 Body Mass Index (BMI)에 따른 본인인지형을 분 류하여 체형인식왜곡(weight misperception)을 분석한 연구들[18,19] 도 부족한 실정이다. 이에 본 연구는 한국 여성의 비만과 왜곡된 체 형 인식이 유방암 검진에 미치는 영향을 확인하고자 시행하였다.
연구 방법
1. 연구 대상
2014년 지역사회 건강조사 자료를 사용하였다. 지역사회 건강조 사는 지역주민의 건강상태를 파악하여 근거에 기초한 보건정책을 수립·평가하기 위한 조사로 매년 시행된다. 인구 전 집단을 모집단 으로 하여 주민등록인구자료와 주택 유형 자료를 참고하여 표본추 출틀을 작성하고 이를 기본으로 보건소별 평균 900명이 조사될 수 있도록 추출되었다. 본 연구에서는 전체 표본 228,712명 중 당시 유 방암학회 암 검진 권고안[20]에 따라 권고 대상인 35세 이상 70세 미 만의 여성을 연구 대상으로 하였다. 의료급여 수급권자는 검진 비 용이 무료이기에 검진행위에 영향을 줄 수 있어 연구 대상에서 제 외하여 총 54,017명의 자료를 바탕으로 연구를 시행하였다.
2. 연구 도구
1) 인구·사회학적 변수
연령은 설문지에 기입한 만 나이를 사용하였고, 최종학력의 경 우, 무학, 초등교육, 중등교육, 고등교육, 대학교육 이상으로 구분하 였다. 가구소득 수준의 경우는 200만 원 미만의 소득, 200만 원 이상 400만 원 미만의 소득, 400만 원 이상의 소득으로 구분하였다. 결혼 상태는 미혼, 기혼 유배우자, 기혼 무배우자(이혼, 별거, 사별)로 범 주화하였다.
2) 체질량지수(BMI)
‘현재 본인의 키는 얼마입니까?’와 ‘현재 본인의 몸무게는 얼마입 니까?’라는 질문에 직접 응답한 데이터를 가지고 BMI 공식 BMI= 체중(kg)/신장2(m2)에 근거, 산출하여 사용하였다. BMI는 18.5 kg/m2 미만을 저체중, 18.5 kg/m2 이상 23 kg/m2 미만을 정상 체중, 23 kg/m2 이상 25 kg/m2 미만은 과체중, 25 kg/m2 이상 30 kg/m2 미만은 비만, 30 kg/m2 이상은 고도비만으로 구분하였다[21].
3) 본인인지체형과 체형인식왜곡
본인인지체형은 ‘현재 본인의 체형이 어떻다고 생각합니까?’라는 질문을 변수로 사용하였다. 이에 대한 응답은 ‘매우 마른 편’, ‘약간 마른 편’, ‘보통임’, ‘약간 비만’, ‘매우 비만’ 다섯 가지이다.
체형인식왜곡은 본인인지체형과 BMI 분류를 이용하여 체형인식 일치군, 과체중왜곡군, 저체중왜곡군 3군으로 구분하였다(Figure 1). 먼저, 체형인식일치군은 BMI 분류와 본인인지체형이 일치한 경 우이다. BMI 분류상 정상 체중 혹은 과체중이면서 ‘보통임’에 응답 한 경우와 BMI 분류상 저체중이면서 ‘매우 또는 약간 마른 편’에 응 답한 경우, BMI 분류상 비만에 속하면서 ‘약간 또는 매우 비만’으로 응답한 경우 체형인식일치군이 된다. 과체중왜곡군은 BMI 분류상 저체중군이나 본인인지체형이 ‘보통’ 혹은 ‘약간 또는 매우 비만’인 경우와 BMI 분류상 정상 체중군이나 본인인지체형을 ‘약간 또는 매우 비만’으로 응답한 경우이다. 마지막으로 저체중왜곡군은 BMI 분류상 비만군이나 본인인지체형이 ‘보통’ 혹은 ‘약간 또는 매우 마 름’인 경우와 BMI 분류상 정상 체중군이나 본인인지체형이 ‘약간 또는 매우 마름’ 인 경우에 해당한다.
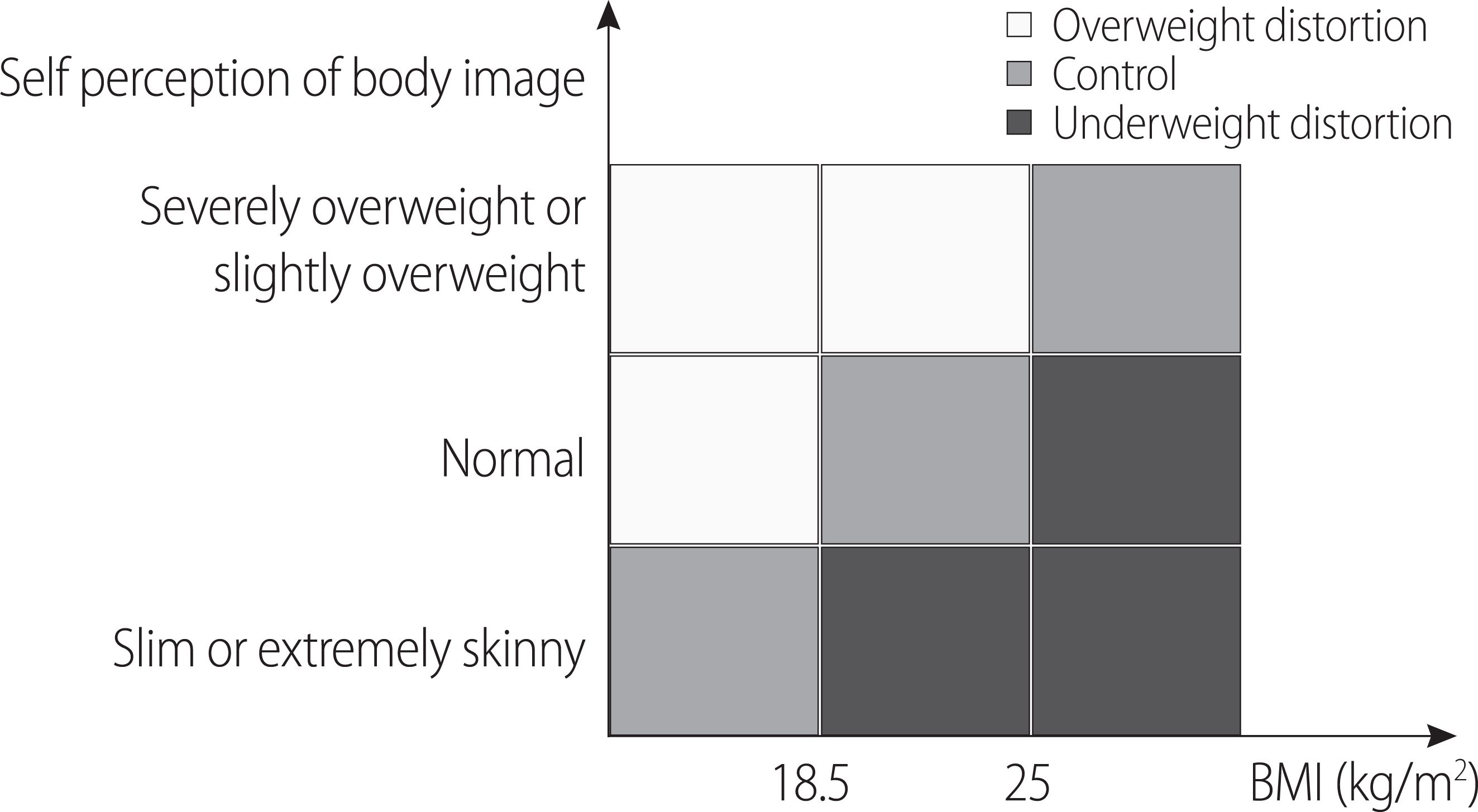
Self perception of body image by body mass index.
4) 건강행동
건강행동의 경우 체중조절행위, 운동, 고위험 음주를 변수로 사 용하였다. 체중조절행위의 경우 ‘최근 1년 동안 몸무게를 조절하려 고 노력한 적이 있습니까?’라는 질문에 대한 응답으로 경험이 있는 경우와 없는 경우로 구분하였다. 운동의 경우, 최근 1주일 동안 격렬 한 신체활동, 중등도 신체활동, 격렬한 신체활동 중 하나라도 하였 다고 응답한 경우 운동을 하는 것으로 보았다. 고위험 음주의 경우, 주 2회 이상 음주를 하며 1회 평균 음주량이 4잔 이상이라고 응답 한 경우 고위험 음주를 하는 것으로 보았다. 흡연의 경우, 현재 흡연 여부에 ‘예’와 ‘아니요’로 나누어 분류하였다.
5) 유방암 검진 수검 여부
유방암 검진 수검 여부는 ‘최근 2년 동안 건강에 특별한 문제는 없 으나 건강상태를 알아보기 위해 유방암 검진을 받은 적이 있습니까?’ 라는 질문에 대한 응답인 ‘예’와 ‘아니요’를 나누어 종속변수로 하였다.
3. 자료 분석
본 연구에서는 R 3.4.1, SAS 9.4 통계 프로그램을 활용하여 분석하 였다. 빈도분석을 통해 연구 대상자들의 인구·사회학적 특성과 건 강행동, BMI, 체형인식왜곡의 분포 확인 후 체형인식왜곡군 별로 각각 교차분석을 하고 카이제곱 검정을 시행하였다. 이후 통계적으 로 유의한 변수들을 통제 후 다중 로지스틱 회귀분석을 사용하여 BMI, 체형인식왜곡이 유방암 검진에 주는 영향을 분석하였다. 통계 적 유의성은 p-value가 .05 미만일 때 유의한 값으로 판정하였다.
4. 윤리적 고려
본 연구는 서울시에 소재한 C대학교 임상연구윤리위원회의 승 인을 받았다(MC17QISI0007). 이후 질병관리본부에 연구자가 서약 서와 개인정보수집 및 이용 동의를 하고 자료 이용 계획서를 작성 하여 자료 요청을 한 후 질병관리본부에서 검토 후 승인을 받아 자 료를 제공받았다.
연구 결과
1. 체질량지수에 따른 체형인식
BMI 분류상 정상 체중이 48.8%로 가장 많았고 과체중 24.3%, 비 만 20.9%이었으며 고도비만은 2.0% 순이었다(Table 1). BMI 18.5 kg/m2 이하의 저체중 군의 24.0%는 본인을 ‘보통 체형’이라고 응답하였 다. 정상 체중군 중 18.5%는 본인 체중을 ‘약간 혹은 매우 비만’이라 고 응답하였다. 과체중군 중 34.6%는 본인 체중을 정상 체중으로 응 답하였다. 비만군 중 10.3%, 고도비만군 중 1.8%는 본인을 ‘보통 체형’ 으로 응답하였다.
Self Perception of Body Image by Body Mass Index (BMI) (N=54,017)
2. 체형인식왜곡군에 따른 일반적 특성
35세 이상 39세 이하에서 과체중왜곡의 비율이 32.2%로 가장 높 았다(Table 2). 연령이 증가할수록 과체중왜곡의 비율은 감소하였 고, 저체중왜곡의 비율은 점차 증가하였다. 특히, 60-69세 저체중왜 곡의 비율은 17.0%로 가장 높았다. 최종학력의 경우 학력 수준이 증 가할수록 과체중왜곡의 비율은 증가하고 저체중왜곡의 비율은 감 소하였다. 무학의 경우 과체중왜곡은 15.3%이었으나 대학 졸업 이 상군은 30.5%이었다. 가구소득 월 400만 원 이상의 집단의 저체중 왜곡비율은 7.4%이고, 월 200만 원 이하의 집단은 13.9%로 차이를 보 였다. 미혼 집단에서 과체중왜곡의 비율이 30.7%로 가장 높았고 저 체중왜곡의 비율은 6.0%로 가장 낮았다.
General Characteristics among Weight Perception Groups (N=54,017)
3. 체형인식왜곡군에 따른 건강행동 특성
체중조절행위의 경우, 경험이 없는 경우가 과체중왜곡군이 15.2%, 저체중왜곡군 18.8% 체형인식일치군 66.0%였다(Table 3). 반대로 체 중조절 경험이 있는 경우는 과체중왜곡군이 31.5%, 저체중왜곡군 4.8%, 체형인식일치군 63.7%로 유의한 차이를 보였다(p < .001). 운동 의 경우에는 하지 않은 집단에서 과체중왜곡군 26.0%, 저체중왜곡 군 9.9%, 체형인식일치군 64.1%이고 운동을 하는 집단에서 과체중왜 곡군 24.0%, 저체중왜곡군 10.1%, 체형인식일치군 65.9%로 유의한 차 이를 보였다(p < .001). 고위험 음주 역시 유의한 차이(p < .001)를 보였 는데, 고위험 음주를 하지 않는 경우는 과체중왜곡군 25.3%, 저체중 왜곡군 10.1% 체형인식일치군 64.6%였으며, 고위험 음주를 하는 경 우에는 과체중왜곡군 32.4%, 저체중왜곡군 5.4%, 체형인식일치군 62.2%였다. 유방암 검진 여부 역시 집단 간 차이를 보였다. 2년 이내 유방암 검진을 하지 않은 집단에서 과체중왜곡군의 비율은 27.9%, 저체중왜곡군은 8.4%였으며 검진을 한 집단에서는 과체중왜곡군 25.2%, 저체중왜곡군 10.1%로 유의한 분포의 차이를 보였다(p < .001).
Health Behaviors among Weight Perception Groups (N=54,017)
4. 한국여성 유방암 검진에 영향을 미치는 요인
나이가 한 살 증가할수록 유방암 검진율은 1.10배(confidence interval, CI: 0.09-0.10, p < .001) 증가하였다(Table 4). 가구소득은 200만 원 미만의 집단에 비하여 200만 원 이상 400만 원 미만의 집단에서 1.15배(CI:0.07-0.21, p < .001)로 높았으며 400만 원 이상의 집단 역시 1.52배(CI: 0.33-0.05, p < .001)로 더 높았다. 결혼 여부의 경우 기혼 유 배우자 집단에 비해 기혼 무배우자 집단의 검진율이 0.90배(CI: -0.18~-0.02, p =.015)로 더 낮았다. 미혼 집단의 경우에는 통계적으로 유의한 영향을 미치지 않았다. 거주 지역의 경우 서울 거주 집단을 기준으로 광역시 거주 집단에서 검진율은 0.81배로 더 낮았다(CI: -0.31~-0.11, p < .001). 도 단위 거주 집단에서도 0.87배(CI: -0.24~-0.05, p =.002)로 더 낮았다. 체중 조절의 경험이 있는 집단의 경우 경험이 없는 집단에 비해 검진율이 1.16배(CI: 0.09-0.21, p < .001) 높았다.
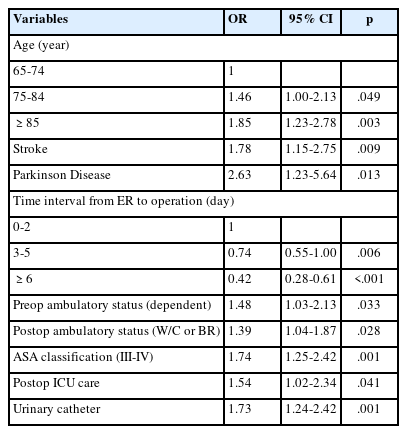
Multivariate Logistic Regression Analysis for Receiving Breast Cancer Screening Test (N=54,017)
BMI가 유방암 검진에 미치는 영향을 살펴보면 과체중군의 유방 암 검진율은 정상체중군에 비해 1.09배(CI: 0.00-0.16, p =.038) 높았 고, 고도비만군은 0.83배 낮았다(CI: -0.36-0.00, p =.047).
체형인식왜곡 역시 유방암 검진에 영향을 미쳤다. 과체중왜곡군 유방암 검진율은 체형인식일치군에 비해 0.93배 낮았다(CI: -0.15- 0.00; p =.037).
논 의
본 연구결과 BMI 18.5 kg/m2 이하의 저체중군의 24.0%는 본인을 ‘보통 체형’이라고 응답하여 저체중임을 인지하지 못하고 있는 것을 알 수 있었다. 정상 체중군 중 18.5%는 본인 체중을 ‘약간 혹은 매우 비만’이라고 응답하였다. 비만(BMI 25 kg/m2 이상)의 비율은 전체의 22.9%에 불과하지만, 응답자 중 45.1%는 본인을 ‘약간 혹은 매우 비 만하다’고 생각하였다. 질병관리본부와 국립보건연구원이 발표한 ‘우리나라 여성의 생애주기별 건강 인식 및 행태조사’에 따르면 중년 여성 42.7%가 본인을 비만하다고 응답하여 본 연구의 결과(45.1%) 와 일치한다[22]. 이는 한국 사회에서 형성된 비만의 기준이 실제 기 준보다 훨씬 엄격함을 시사한다.
다음으로 유방암 검진에 영향을 미치는 요인을 살펴보면, 선행연 구와 같이 인구 사회학적 특성에 따라 유방암 검진에 격차가 존재 하였다. 먼저, 연령이 높을수록 검진 확률이 증가하였는데 이는 40 대를 기준으로 나이가 증가할수록 검진율이 증가하는 선행연구 [23]와 일치하였다. 이는 만 35세부터 유방암 검진이 권고되나 만 40 세부터 국가 검진 혜택을 받는 것이 영향을 미친 것으로 보인다.
교육수준의 경우 무학에 비해 교육수준이 높은 집단이 유방암 검진의 교차비가 높았는데, 이는 서울시 성인 거주자를 대상으로 한 연구에서 교육수준에 따라 뚜렷한 계단형의 수진율이 나타난 Chun [24]의 결과와 유사하였다. 이는 교육을 통해 습득한 지식과 기술은 건강검진을 비롯한 예방적 건강행동을 하는 데 영향을 미 칠 뿐만 아니라 개인의 교육수준과 배경은 경제적 수준과 밀접한 관련성을 가지므로[25] 큰 설명력을 갖는 것으로 보인다.
가구소득 역시 중요한 영향 요인이다. 가구소득이 높을수록 유 방암 수검 가능성은 증가하였다. Chun [24]의 연구에 따르면 월평균 가구소득 최상위 집단의 odds ratio는 1.73으로 차이가 존재하였다. 그러나 1997년에 비해 2005년의 여성의 건강검진 수검에 대한 소득 수준 교차비가 시계열분석에서 통계적으로 유의하게 줄어들었다. 일반적으로 의료이용은 경제적 구매 능력에도 크게 의존하기 때문 에[25] 소득이 높을수록 의료이용의 일종인 유방암 검진 수검의 가 능성이 상승하게 되는 것으로 보인다. 다만, Chun [24]은 이러한 차 이가 조금씩 줄어든 것이 국가의 저소득층의 의료접근성을 강화하 는 정책이 긍정적으로 작동한 것으로 예상하였다.
건강행동의 경우 규칙적인 운동을 하거나 다이어트 경험이 있는 경우 유방암 검진을 더 많이 하는 것으로 나타났다. 이는 규칙적인 운동을 많이 할수록 유방암 검진 수검의 교차비가 높아진다는 선 행연구와 일치하는 결과이다[26]. 대개 건강한 생활습관을 실천하 는 사람들이 건강검진을 이행하게 된다는 연구결과가 있는 만큼 [15,16] 건강행동 역시 유방암 검진에 영향을 미치는 것으로 보인다.
본 연구결과 비만 여부와 체형인식왜곡의 경우 모두 유의하게 유 방암 검진에 부정적인 영향을 끼침을 확인할 수 있었다.
본 연구에서는 BMI를 기준으로 과체중군은 정상체중군에 비해 검진 확률이 증가하였고 고도비만군은 감소하였는데, 이는 고도비 만 집단에서 유방암 검진 확률이 감소한 선행연구[17]의 결과와 일 치한다.
또한 체형인식왜곡은 비만보다 유방암 검진에 더 큰 설명력을 가 졌다. 체형인식일치군에 비하여 과체중왜곡군의 경우 검진 가능성 이 감소한 반면, 저체중왜곡군의 경우에는 영향을 주지 않는 것으 로 나타났다. 이는 부정적 신체이미지를 갖는 집단이 암 검진을 회 피한다는 선행연구와도 일치한다[12]. 또한 비만으로 인한 차별 경 험은 운동과 같은 건강행동을 회피하게 한다는 결과[27]나 비만할 수록 의료이용을 꺼린다는 선행연구[28]와도 맥락을 같이한다. 다 시 말해, 고도비만인 사람이나 과체중왜곡군의 경우 유방암 검진 가능성이 감소함에 따라 한국의 엄격한 ‘비만’ 기준이 예방적 건강 행동에 장애물로 작용할 수 있다. 특히 과체중왜곡군은 실제 비만 이 아니지만, 비만하다고 느끼는 집단이므로 실제 비만이 아닌 비 만에 대한 인식이 유방암 검진에 부정적 영향을 끼침을 시사한다.
본 연구는 방법론적으로 몇 가지 한계점을 가진다. 먼저, 부족한 변수로 연구의 해석에 제한이 있다는 점이다. 비만 집단이 인지하 는 혹은 인지하지 못하는 낙인, 의료 현장에서의 차별 경험이나 미 디어나 혹은 정책적으로 전달하는 ‘반-비만 메시지’들은 대규모 2차 자료에서는 조사되지 않는 변수이다. 후속연구에서는 질적 연구, 양 적 연구를 모두 통합하는 mixed-method 연구 방법을 적용해 양적 연구에서는 드러나지 않는 비만 집단의 건강행동 영향요인을 탐구 할 필요가 있다.
둘째, BMI를 산출하는 데 있어서 실측치가 아닌 자기기입형식으 로 조사한 것이기 때문에 BMI가 실측치와 다르게 나타날 수 있다. 따라서 주요 독립변수인 BMI와 본인인지체형을 바탕으로 한 체형 인식왜곡변수가 실제와 다르게 나타날 수 있다. 또한, 회상 비뚤림 (recall bias)으로 인하여 최근 2년 이내의 유방암 수검 여부를 묻는 종속변수가 실제와 차이가 있을 수 있다.
셋째, 지역사회건강조사는 매년 조사되는 횡단면 조사이다. 따라 서 한 시점에서 현황을 파악하고 관련 변수 간의 관련성이 있는지 를 알 수는 있지만, 인과관계를 파악하기 어렵다.
그럼에도 본 연구는 비만 집단에 보이지 않는 장애요소가 분명 히 존재함을 대규모 계량 연구를 통해 실증적으로 검증하였다는 점에서 의의가 있다. 비슷한 주제를 다룬 연구들이 대부분 일부 지 역을 대상으로 한 설문조사임에 반하여 본 연구는 인구 전 집단을 모집단으로 하여 비례 및 계통 추출된 표본을 대상으로 분석한 연 구라는 점에서 대표성을 획득할 수 있는 연구라고 생각된다. 아울 러 체형인식왜곡 여부가 유방암 검진 수검에 미치는 영향을 대규모 2차 자료를 이용하여 분석한 연구로는 국내 최초의 연구라는 점에 서 의의가 있다.
결 론
본 연구는 여성의 비만 혹은 체형인식왜곡이 유방암 검진 수검 에 장애물로 작용함을 입증한 연구이다. 이를 바탕으로 비만 여성 에 대한 건강행동 독려 및 의료현장에서의 고립을 해결하기 위한 중재 방향을 제시한다면 다음과 같다.
먼저, 사회적 규범인 비만과 신체 이미지의 개념이 사회에서 다시 ‘구상’되어야 한다. 비만하지 않은 여성들의 상당수가 본인을 비만 으로 인식하고 있다. 그러나 실제 비만 여부와 상관없이 부정적 신 체왜곡이 심할수록 유방암 검진을 하지 않음을 본 연구를 통해 확 인할 수 있었다. 선행연구들에 따르면 ‘비만’이라고 생각하는 사람 은 자기효능감이 떨어지고 신체 회피를 하거나 신체 노출에 수치심 을 느끼게 되어 검진을 하지 않을 가능성이 더욱 커지게 된다[12]. 이 러한 기전에는 사회에서 ‘비만’을 어떻게 보느냐가 크게 작용하게 된다. 오히려 엄격한 비만의 기준이 체형인식왜곡을 심화시키고 건 강행동에 장애물로 작용할 수 있음을 유의해야 할 것이다.
또한, 사회적 측면에서 비만 집단에 대한 편견을 심화시키는 ‘반- 비만 메시지’는 사라져야 할 것이다. Puhl 과 Brownell [29]의 사회 합 의적 접근에 따르면, 비만과 같이 가시적으로 두드러지는 집단에 대한 편견과 낙인은 사회적 합의에 따라 구상된다. 반대로 이를 감 소시키는 것 또한 사회적으로 구상될 수 있다. 그러나 아직도 많은 연구에서 비만을 개인 수준의 문제로 치부하고 있다. 의료현장에서 아직도 비만을 ‘일탈행위’로 간주한 메시지가 비만을 해결하는 전 략으로 사용되기도 한다[30]. 그러나 이러한 메시지들은 비만 여성 을 ‘일탈 여성’으로 스스로를 내재화하여 본 연구에서처럼 건강행 동을 하는 데 장애물로 작용할 수 있다. 따라서 의료현장에서 간호 사는 비만 차별적 태도를 지양하고 커뮤니케이션 과정에서 비만 집 단에 대한 편견을 증폭하는 메시지를 포함하고 있지는 않은지 항 상 유의해야 한다.
인구 사회학적 특성 외에도 비만 혹은 과체중인식왜곡만으로도 유방암 검진 수검에 영향을 미칠 수 있음이 밝혀진 만큼 보다 세밀 한 독려 전략이 요구된다. 그러나 아직은 이에 관련한 연구가 부족한 실정이다. 이를 위해 본 연구에서 밝혀진 고도비만 집단과 과체중인 식왜곡집단을 대상으로 한 후속연구를 통해 이들 집단의 암 검진에 영향을 끼치는 요인이 무엇인지 보다 면밀히 파악해야 할 것이다.
CONFLICT OF INTEREST
No conflict of interest has been declared by the authors.