
INTRODUCTION
Sepsis is a life-threatening condition caused by suspected or apparent infection. The annual incidence of sepsis is about 50 million globally, and sepsis-related mortality is 25%-30% [1]. Sepsis has ranked top among the most expensive conditions treated in the United States, and the annual medical cost of sepsis in the US is $24 billion [2]. In Korea, the mortality rate from sepsis has nearly tripled in 10 years and is the 10th leading cause of death for women [3]. Sepsis causes multiple organ damages at the molecular and cellular level, such as changes in inflammatory signals and metabolic disorders, as well as organ levels, including microcirculation changes and endothelial changes [4], and can lead to septic shock and death if left untreated. However, those unwanted critical conditions can be prevented by early detection [5]. If sepsis is detected within an hour and treated in a timely manner, the prevalence, mortality, and total medical expenses of this critical and costly condition can be reduced [6]. Nevertheless, early recognition is not easy because initial symptoms of sepsis are nonspecific and ambiguous. In addition, health care professions’ lack of knowledge of sepsis has been reported [7-9].
Nurses are health care workers who take care of patients at bedside, and spend more time by patients than any other professions. Therefore, it is very critical for nurses to assess sepsis quickly in order to avoid serious consequences. In order to assess patients accurately and fast, there is need for effective educational intervention [8]. Studies on sepsis knowledge and education programs have been focused more on nurses working at intensive care units [8,10]. However, the place where initial changes of patients’ clinical manifestations take place is in general units rather than intensive care units. A significant number of sepsis patients were treated in general units [11]. Unfortunately, it is reported that nurses working at general units have poor knowledge of sepsis recognition and initial intervention [12]. Thus, education programs targeting them are compelling.
For proper recognition and initial intervention on sepsis, it is important to understand current sepsis guidelines and to utilize standardized screening tools in addition to general understanding of sepsis. However, most nurses did not follow current guidelines on sepsis due to lack of knowledge [7]. Therefore, it is also essential to educate nurses the guidelines and screening tools to use them properly and adhere them persistently.
The third international consensus definitions for sepsis and septic shock (Sepsis-3) were announced in 2016 by a joint collaboration of the Society of Critical Care Medicine and the European Society of Intensive Care Medicine [13]. Sepsis-3 introduced SOFA and quick SOFA (qSOFA) criteria for identifying sepsis and septic shock. The qSOFA is a bedside clinical score without laboratory test, thus it can be rapidly and repetitively scored by nurses at the bedside. It is reported that educational programs with screening tools especially the sepsis-related Sequential Organ Failure Assessment (SOFA), decrease mortality and medical expenses due to sepsis and increase survival [14].
Although there is a significant relationship between education and knowledge, knowledge and performance are not always related [15]. Therefore, an educational approach helpful for a transition from knowledge to practice should be adopted in order to improve both knowledge and practice. Among various effective education methods, case-based learning is constructed on the basis of patient cases and focuses on clinical-based knowledge [16]. Case-based learning has been known to be effective in nursing education and globally utilized. In addition, case-based learning is more effective in improving critical thinking and assessment skill and applying theory in practice than traditional lecture [17]. Therefore, case-based learning is considered to be an effective education method for clinical nurses to increase knowledge and assessment skill. Education is known to increase self-efficacy. There are evidences that case-based learning also increases self-efficacy of health care professions [18]. Self-efficacy is one of the influential factors on motivation and behavior [19]. For example, the nurses with high perceived self-efficacy are more motivated to apply knowledge and skills in practice. Therefore, knowledge, skill, and self-efficacy are related to each other.
With advances in information technology, mobile devices, such as smartphones, have been used in clinical training and practice. Among types of applications in mobile devices, guidelines, algorithm, and calculators are commonly used [20,21]. It shows that use of mobile devices in practice improves accuracy and confidence, while also reducing errors [22,23]. Regarding sepsis, there are mobile applications providing sepsis criteria and calculating SOFA and qSOFA scores on patients’ clinical and laboratory data in the application markets. In the consideration of complexity of sepsis criteria, utilization of applications may improve recognition of sepsis.
In this study, we tested the effects of educational intervention on sepsis with case-based learning option (case-based sepsis education) and the use of a smartphone application with case-based sepsis education on the knowledge, accuracy of sepsis assessment, and self-efficacy of nurses working at general units. In addition, we identified the relationship between knowledge, accuracy of sepsis assessment, and self-efficacy.
METHODS
Design and Sample
A quasi-experimental pretest-posttest design with a control group was used for this study. The sample size was 20 for each group, for a total of 60 participants, calculated based on power=0.8, effect size=0.4, and alpha=0.05. According to the study of Delaney, Friedman [24], which is similar to our study, the effect size d was 2.39, which is a “large” effect size. Because we used the repeated measure ANOVA test, we needed an effect size f instead of d. Therefore, we used 0.4 for effect size to calculate the sample size, because 0.4 is categorized to “large” effect size for f. In consideration of missing rates, 60 participants were recruited by convenient sampling from eighteen non-critical care units at a tertiary medical center in Seoul, Korea. Nurses working at pediatric units were excluded because the definition of sepsis differs from adults in children. We collected data from all 60 participants finally without dropout (Figure 1).

Measurements
Knowledge of sepsis
Jin [25] developed a questionnaire consisting of 33 items to measure knowledge of sepsis for nurses working at intensive care units. Because Jin’s questionnaire was based on the previous version of sepsis guideline, we modified the questionnaire based on new sepsis guidelines and the opinions of experts consisting of a physician, an infection control nurse, and a nursing professor. A total of 30 items with a Content Validity Index (CVI) value of 1.0 were finally included in the questionnaire. Total scores of correct answers were converted to a percentage. The reported Kuder-Richardson 20 (KR-20) by Jin was .72 while KR-20 in this study was .86. The higher scores indicate better knowledge of sepsis.
Accuracy of sepsis assessment
To measure accuracy of sepsis assessment, case scenarios were developed as the first step. Each case provides information on past health history, present health history, clinical manifestations, and laboratory data. To prevent case scenarios from being exposed to other groups, different sets of case scenarios were developed for each group. Content validity was confirmed by a physician, an infection control nurse, and a nursing professor. For each case, the experts checked whether the contents of the case fit the purpose, and whether it was appropriate in terms of clinical relevance and difficulty. As a result, 28 cases had a CVI of 1 point and two cases had a CVI of .67. The results of re-validation after revising the two items, the final CVI was 1. Three question items were included in each case to measure accuracy. Each set consisted of 10 cases and 30 question items. Finally, a total of three sets of case scenarios and questions were established. The similarity in difficulty levels of case scenarios among groups were validated by experts based on data such as chief complaint, physical examination, laboratory test results, and vital sign. The final CVI of difficulty level of cases among three group was 1. Each set of 10 cases was randomly assigned to the control, intervention I, or intervention II groups. Total scores of correct answers were converted to a percentage. The KR-20 of the accuracy scale in this study was .91. The higher scores indicate higher accuracy of sepsis assessment.
Self-efficacy for nursing care of sepsis
The self-efficacy scale originally developed by Sherer et al. [26] and translated into Korean by Yang [27] was modified to assess self-efficacy on sepsis nursing care. Content validity was confirmed by three experienced nurses with master’s degrees. The CVI value of 12 items was 1.0, while the value of two items was .67. The two items were revised to reflect the opinion that the conveying of meaning was ambiguous. After wording revising the wording for two items, the scale was re-evaluated by the experts, and the CVI value of all 14 items was 1.0. Therefore, all 14 items with a 4-point Likert scale were finally included in the questionnaire. The higher the scores, the better the self-efficacy was. Cronbach’s alpha of this questionnaire in this study was .90 while the reported Cronbach’s alpha by Yang (1999) was .79.
Case-Based Education Program on Sepsis
The case-based education program in this study was developed based on literature reviews and experts’ opinions. The contents of the educational materials included a general understanding of sepsis, the latest sepsis guidelines, and sepsis assessment including SOFA and qSOFA criteria for all groups. The general understanding of sepsis consisted of definition, epidemiology, pathophysiology, clinical manifestations, and the general concept of the Hour-1 bundle. Sepsis guideline information included initial resuscitation, antibiotic therapy, fluid therapy, vasopressors, transfusion, other supportive therapy, and sepsis algorithm.
For the intervention groups, a case-based learning session was included. The cases used in the session were developed based on sepsis patients’ records and literature reviews. The cases provided detailed patient information including age, gender, past and present health history, chief complaints, results of physical assessment, and laboratory test results. Initially, the participants were taught step by step how to detect the patient’s status regarding sepsis in group. Then the cases were provided to the individual participants to assess the patients in the scenario. The correct assessment of the four cases in the scenario was “1 qSOFA point with non-septic status”, “2 qSOFA points with non-septic status”, “2 qSOFA points with septic status”, and “3 qSOFA points with septic shock.” Debriefing was followed after assessment.
In the intervention I group, the participants were asked to memorize qSOFA and SOFA criteria prior to their case-based learning session. For the intervention II group, the participants were asked to install the smartphone application (SEPSIS 3, ScyMed Inc., Houston Texas, US) providing items of qSOFA and SOFA criteria and having functions to calculate qSOFA and SOFA scores automatically when values were filled in for each of the items. Among the several sepsis-related applications, SEPSIS 3 was chosen because it is available for both iPhone and android phones and the latest information was well reflected. The validity of the application was tested with data and the guidelines. The intervention II group assessed the septic status of four cases using the application.
Procedures
Eighteen units were assigned to the control, intervention I, or intervention II groups by matching unit characteristics. Study participants were recruited using bulletin boards and the Internet. To prevent contamination of treatment, interventions were provided per units. Pretests including knowledge of sepsis, accuracy of sepsis assessment, and self-efficacy on sepsis management were done prior to the educational program. For the control group, self-learning was done by providing a booklet containing the same education contents except case-based information. Case-based learning program was performed by a researcher to both intervention groups, but the smartphone application with qSOFA and SOFA calculation function was provided only to intervention II group. The education time was about 50 minutes per group. Immediately after education, posttests on knowledge, accuracy of sepsis assessment, and self-efficacy were performed. Data were collected from April to July, 2019.
Data Analysis
IBM SPSS Statistics Version 25.0 (IBM, Chicago, IL) was used for statistical analyses and Jamovi version 1.2.22 [28] was used for density and correlation matrix plots. Data were summarized using means, standard deviation, frequency, and percentage. The Kolmogorov-Smirnov and Shapiro-Wilk tests were performed to test normality. To test homogeneity among groups, a one-way analysis of variance (one-way ANOVA) or Kruskal Wallis test was used depending on normality. For categorical variable, chi squared test was used. When the observation was less than 5, the exact test of the Fisher was performed instead of the chi-square test. To test differences in knowledge, accuracy of sepsis assessment, and self-efficacy on sepsis between groups across time, a mixed design ANCOVA for parametric analysis, or generalized estimating equations (GEE) for nonparametric analysis, was applied because a few general characteristics were different among groups. Post-hoc tests utilized in this study was one-way ANCOVA, Wilcoxon signed rank test, Kruskal Wallis test, or Mann-Whitney test. To examine the relationships between knowledge, accuracy of sepsis assessment, and self-efficacy, correlation was analyzed using Spearman’s rho due to failure of normality. The level for statistical significance was at a p value less than 0.05. Bonferroni’s correction was used to adjust for multiple comparisons.
Ethical Considerations
This study was approved by the Institutional Review Board of Samsung Medical Center (No 2019-03-092). All participants were informed of the purpose of study and told that their responses would be kept confidential and that the results of the study would be used only for the purposes of the study. The participants were also given the option to withdraw from the study at any time. Signed consent forms were obtained from the participants after the full explanation of the process.
Results
Characteristics of Participants
The demographic and sepsis-related characteristics of the participants are presented in Table 1. Most participants were female (95%), single (80%), and had a bachelor’s degree (93%). Most of them had experience in caring for a sepsis patient, but three-quarters of them did not have sepsis education after graduation. Approximately a half of them experienced a delay in detection of sepsis, while almost two-thirds of the participants said that they were not able to detect sepsis well. Furthermore, only a few participants responded that they knew about the SOFA and qSOFA criteria. There was no difference in demographic and sepsis-related characteristics among the three groups, except for age, years of clinical experience, and marital status. Those differences were counted as covariance variables when analyzing the effect of intervention.
Table 1.
General and Sepsis-related Characteristics (N=60)
| Variable | Total (n=60) | Control (n=20)a | Intervention I (n=20)b | Intervention II (n=20)c | F or χ2 | p | ||||
|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
|
|||||||
| Mean or n | SD or % | Mean or n | SD or % | Mean or n | SD or % | Mean or n | SD or % | |||
|
|
||||||||||
| Age (yr) | 26.92 | 3.12 | 28.55 | 2.48 | 26.3 | 2.98 | 25.9 | 3.3 | 12.53 | .002 |
| (a>b,c) | ||||||||||
| Clinical experience (yr) | 3.83 | 3.08 | 5.19 | 2.9 | 3.34 | 2.79 | 2.95 | 3.22 | 9.11 | .01 |
| (a>b,c) | ||||||||||
| Gender | 0.47 | 0.791 | ||||||||
| Male | 3 | 5 | 0 | 0 | 1 | 1.7 | 2 | 3.3 | ||
| Female | 57 | 95 | 20 | 33.3 | 19 | 31.7 | 18 | 30.0 | ||
| Marriage | 7.38 | .025 | ||||||||
| Single | 48 | 80 | 12 | 20 | 18 | 30.0 | 18 | 30.0 | (a>b,c) | |
| Married | 12 | 20 | 8 | 13.3 | 2 | 3.3 | 2 | 3.3 | ||
| Educational level | 0.53 | .768 | ||||||||
| Associate degree | 1 | 1.7 | 1 | 1.7 | 0 | 0 | 0 | 0 | ||
| Bachelor’s degree | 56 | 93 | 17 | 28.3 | 20 | 33.3 | 19 | 31.7 | ||
| Master’s or higher | 3 | 5 | 2 | 3.3 | 0 | 0 | 1 | 1.7 | ||
| Unit characteristics | 0.47 | .791 | ||||||||
| Medical | 42 | 70 | 14 | 23.3 | 15 | 25 | 13 | 21.7 | ||
| Surgical | 18 | 30 | 6 | 10 | 5 | 8.3 | 7 | 11.7 | ||
| Sepsis education | 2.10 | .350 | ||||||||
| No | 45 | 75 | 15 | 25 | 17 | 28.3 | 13 | 21.7 | ||
| Yes | 15 | 25 | 5 | 8.3 | 3 | 5 | 7 | 11.7 | ||
| Nursing experience on sepsis patients | 0.24 | .889 | ||||||||
| No | 10 | 16.7 | 3 | 5 | 3 | 5.0 | 4 | 6.7 | ||
| Yes | 50 | 83.3 | 17 | 28.3 | 17 | 28.3 | 16 | 26.7 | ||
| Experience in delayed detection in sepsis | 0.41 | .815 | ||||||||
| No | 36 | 60 | 13 | 21.7 | 11 | 18.3 | 12 | 20.0 | ||
| Yes | 24 | 40 | 7 | 11.7 | 9 | 15 | 8 | 13.3 | ||
| Perceived capability to detect sepsis | 3.73 | .444 | ||||||||
| Strongly not capable | 10 | 16.7 | 1 | 1.7 | 5 | 8.3 | 4 | 6.7 | ||
| Not capable | 27 | 45.0 | 9 | 15 | 9 | 15.0 | 9 | 15.0 | ||
| Capable | 23 | 38.4 | 10 | 16.7 | 6 | 10.0 | 7 | 11.7 | ||
| Strongly capable | 0 | 0 | 0 | 0 | 0 | 0.0 | 0 | 0 | ||
| Subjective knowledge level on qSOFA | 5.95 | .429 | ||||||||
| Strongly not knowledgeable | 40 | 66.7 | 11 | 18.3 | 13 | 21.7 | 16 | 26.7 | ||
| Not knowledgeable | 18 | 30.1 | 7 | 11.7 | 7 | 11.7 | 4 | 6.7 | ||
| Knowledgeable | 1 | 1.7 | 1 | 1.7 | 0 | 0 | 0 | 0 | ||
| Strongly knowledgeable | 1 | 1.7 | 1 | 1.7 | 0 | 0 | 0 | 0 | ||
| Subjective knowledge level on SOFA | 6.91 | .329 | ||||||||
| Strongly not knowledgeable | 42 | 69.9 | 11 | 18.3 | 14 | 23.3 | 17 | 28.3 | ||
| Not knowledgeable | 16 | 26.7 | 7 | 11.7 | 6 | 10 | 3 | 5 | ||
| Knowledgeable | 1 | 1.7 | 1 | 1.7 | 0 | 0 | 0 | 0 | ||
| Strongly knowledgeable | 1 | 1.7 | 1 | 1.7 | 0 | 0 | 0 | 0 | ||
Knowledge of Sepsis
There were significant differences in knowledge between groups (χ2=21.69, p<.001) and within the groups over time (χ2=339.57, p<.001). The interaction between the groups and time was significant as well (χ2=50.07, p<.001; Table 2). According to post-hoc tests on time effects, posttest knowledge scores in the control, intervention I and intervention II groups (Median (IQR)=68.34 (15.83), 90.00 (6.66), and 96.67 (3.34), respectively) increased compared to pretest (Median (IQR)=45.00 (16.66), 36.67 (26.67), and 50.00 (17.50) ; p<.05, respectively). In terms of group difference, knowledge scores on sepsis in the intervention I group were significantly higher compared to the control group (U=34.5, Z=-4.49, p<.001). The knowledge in the intervention II group was also improved compared to the control group (U=45.50, Z=-4.19, p<.001). However, there was no statistically significant difference between the intervention I and II group (U=155.0, Z=-1.22, p=.231). For visualization in changes between pre- and posttest by group, density plots are presented in Figure 2.
Table 2.
Effects of Educational Intervention on Knowledge, Accuracy of Sepsis Assessment, and Self-efficacy
| Outcome variable | Control (n=20) | Intervention I (n=20) | Intervention II (n=20) | F or χ2 p | t or U p | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
|
|
||||||||
| Mean | SD | Mean | SD | Mean | SD | Group | Time | Interaction between Group and time | Control vs. Intervention I | Control vs. Intervention II | Intervention I vs. Intervention II | |
|
|
||||||||||||
| Knowledge on sepsis | ||||||||||||
| Pretest Mean, SD | 43.33 | 17.77 | 36.83 | 17.15 | 47.83 | 19.83 | 21.69 | 339.57 | 50.07 | 34.50 | 45.50 | 155.0 |
| Posttest Mean, SD | 64.17 | 13.84 | 88.83 | 5.54 | 94.83 | 3.82 | ||||||
| Difference Mean, SD | 20.83* | 13.55 | 52.00* | 17.68 | 47.00* | 19.85 | <.001 | <.001 | <.001 | <.001 | .231 | |
| Accuracy of sepsis assessment | ||||||||||||
| Pretest Mean, SD | 35.50 | 32.05 | 23.83 | 17.78 | 38.00 | 30.96 | 33.92 | 555.69 | 85.98 | 26.50 | 63.00 | 186.5 |
| Posttest Mean, SD | 53.33 | 12.04 | 86.50 | 5.13 | 97.67 | 2.67 | ||||||
| Difference Mean, SD | 17.83* | 26.67 | 62.67* | 19.39 | 59.67* | 30.38 | <.001 | <.001 | <.001 | <.001 | <.001 | .718 |
| Self-efficacy | ||||||||||||
| Pretest Mean, SD | 40.6 | 6.20 | 39.2 | 5.11 | 37.80 | 5.60 | 1.49 | .001 | 17.47 | 6.19 | 6.00 | 1.31 |
| Posttest Mean, SD | 41.85 | 5.27 | 46.3 | 3.87 | 46.07 | 4.77 | ||||||
| Difference Mean, SD | 1.25 | 2.51 | 7.10* | 3.40 | 8.90* | 5.12 | .234 | .98 | <.001 | <.001 | <.001 | .180 |

Accuracy of Sepsis Assessment
There were significant differences in accuracy between groups (χ2=33.92, p<.001) and time (χ2=555.69, p<.001). The interaction between group and time was significant as well (χ2=85.98, p<.001; Table 2). The posttest accuracy of sepsis assessment in the control, intervention I and intervention II groups (Median (IQR)=55.00 (19.17), 86.67 (9.17), and 98.34 (3.33), respectively) was improved compared to pretest (Median (IQR)=21.67 (35.00), 20.00 (19.17), and 26.67 (40.00), respectively; p <.05). Sepsis assessment in the intervention I group was statistically significantly more accurate than the control group (U=26.50, Z=-4.70, p<.001). The accuracy in the intervention II group was significantly better than the control group as well (U= 63.00, Z=-3.71, p<.001). However, there was no statistically significant difference between the intervention I and intervention II groups (U=186.50, Z=0.37, p=.718).
Self-Efficacy for Nursing Care of Sepsis
There was no statistically significant difference in the self-efficacy among the groups (F=1.49, p=.234) and over time (F=0.001, p=.980), while there was a significant difference in interaction (F=17.47, p<.001). There was no difference between pre- and posttest in the control group (mean±SD=40.60±6.20 and 41.85±5.27, respectively; p=.096), while there were differences between pre- and posttest in both the intervention I (mean±SD=39.20±5.11 and 46.30±3.87, respectively; p<.05) and II (mean±SD=37.80±5.60 and 46.07±4.77, respectively; p<.05) groups. The self-efficacy of the intervention I and II groups was statistically significantly higher than the control group (t=6.19, p<.001; t=6.00, p<.001, respectively), while there was no statistically significant difference between the intervention I and intervention II groups (t=1.31, p=.180).
The Relationship between Knowledge, Accuracy of Sepsis Assessment, and Self-Efficacy
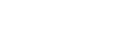
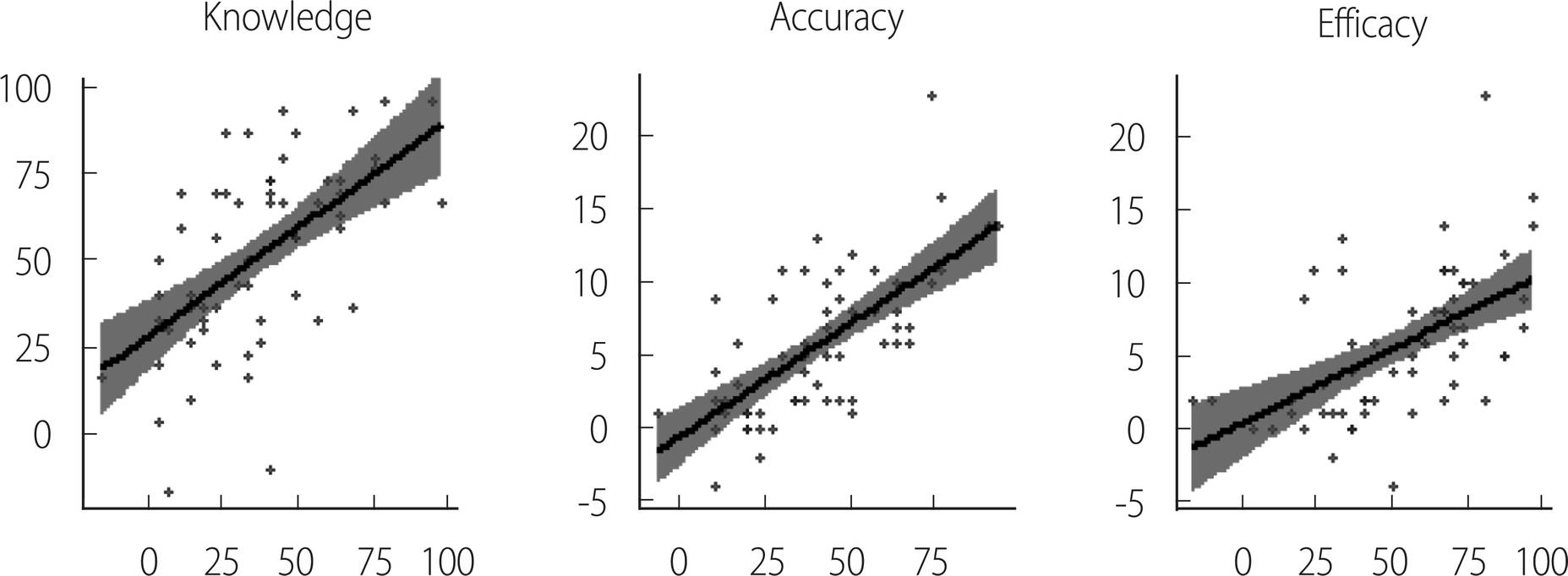
A Spearman’s rank-order correlation was done to identify the relationship between the 60 participants’ knowledge and accuracy of sepsis assessment. There was a moderate, positive correlation between knowledge and accuracy of sepsis assessment, which was statistically significant (rs=.60, p<.001; Figure 3). There was a relatively strong, positive relationship between knowledge and self-efficacy (rs=.67, p<.001), while there was a moderate, positive correlation between accuracy of sepsis assessment and self-efficacy (rs=.57, p<.001).
DISCUSSION
This study examined a case-based sepsis education on nurse’s knowledge, accuracy of sepsis assessment, and self-efficacy, with or without a smartphone application with sepsis algorithm functions. We examine the relationship between knowledge, accuracy of sepsis assessment, and self-efficacy as well. The participants in this study were working at non-ICU adult care units. Most of the participants had experience in taking care of sepsis patients, but the number of nurses who received sepsis education was relatively small. Almost half of them reported that they encountered a delayed recognition of sepsis, and two-thirds of them perceived that they were not able to detect sepsis confidently. These results are comparable with other studies showing lack of knowledge of nursing working in non-intensive care units [7,12]. Therefore, knowledge deficit in sepsis due to lack of educational opportunities is apparent in nurses working in general units, and educational programs for them is in need.
We will discuss effects of the case-based sepsis education first, and then the effect of a mobile application later. In this study, knowledge of sepsis improved significantly compared to baseline regardless of the group. The reason is that all groups were involved in learning about sepsis. Even in the control group, participants learned about sepsis with the provided sepsis education booklet, which has the same information as the intervention groups, except the case-based learning. Therefore, regardless of learning methods, education improves knowledge of sepsis. This result is consistent with other studies regarding sepsis education [10,24,29,30]. However, both case-based sepsis education programs showed more significant improvement in knowledge than the control group did. The effect of the case-based education program on sepsis has not been published yet to our knowledge, but the results of this study are similar to other studies on knowledge improvement with case-based learning in health care fields [31,32]. It is suggestive that case-based education is an effective method to increase knowledge of sepsis.
The participants in our study presented an increase in accuracy of sepsis assessment as well as knowledge regardless of group. Similar with knowledge, nurses in both intervention groups assessed more accurately after intervention compared to the control group. The intervention groups obtained information on sepsis first, then practiced sepsis assessment with case-based learning. The learning experience improved both knowledge and accuracy of sepsis assessment even though the case-based learning was done in a short time. This is congruent with another study [32] in which case-based learning enhanced knowledge and nursing outcomes, irrespective of the methods to provide it. It is also consistent with a study which case-based learning improved dental students’ diagnostic skill [33], and a study that it increased decision making and critical thinking of nursing students [34]. Therefore, it is suggestive that case-based learning may be effective to improve knowledge and accuracy of sepsis assessment. In addition, it may be worth trying even for a short time depending on the topic.
In this study, perceived self-efficacy increased after education in the intervention groups, but not in the control group. It suggests that self-study without case-based learning is not effective to improve self-efficacy, while case-based learning does enhance self-efficacy. There are controversial perspectives on self-efficacy and case-based learning. Roshangar, Azar [18] reported that case-based learning improved critical thinking of nursing students, while not increasing self-efficacy. However, self-efficacy is improved when combining conceptual mapping with case-based learning in their study. The difference in effects on self-efficacy may derive from the following characteristics: Our study measured functional self-efficacy on sepsis care in nurses, while the study of Roshangar, Azar [18] targeted nursing students and measured academic self-efficacy. A qualitative focus group study presented an improvement in self-confidence in practice and recognition of clinical situations through case-based learning [35]. Kantar&Massouh did not use the term “self-efficacy” specifically, but self-confidence and self-efficacy are similar terms in the context of their description. Although the differences are generated from discrete topics, participants, and outcome measures, the effects of case-based learning on self-efficacy need further investigation.
We also utilized a smartphone application in case-based learning in this study. Applications for smartphones have increased in healthcare fields. They are used as platforms for educational materials or tools for practice [36]. In our study, we used an application as a tool for guide references and as a calculator based on guideline algorithms. The intervention I group was exposed to case-based learning after memorizing sepsis detection algorithms and tools including qSOFA and SOFA criteria, while intervention II group used a smartphone application without memorizing the content. There was no difference between intervention group I and II in knowledge, accuracy of sepsis assessment, and self-efficacy. This result suggests that the use of the application had a similar outcome to the acquisition of knowledge through memorization. Therefore, it is beneficial and convenient to apply it on a problem that does not occur often, which may make it difficult for nurses to retain the details. Real-time electronic surveillance in an electronic medical record system would be better than a smartphone application [37]. However, the real-time surveillance system is not available and feasible in all clinical settings. On the contrary, smartphone applications can be obtained for free or low costs. Therefore, the use of applications seems cost-effective.
Previous studies show that the use of applications is effective for nursing students in reducing mistakes and enhancing self-efficacy. For example, junior nursing students using an application providing drug information and a clinical calculator are more accurate and faster in calculating doses and making clinical decisions in medication administration [23]. The study of Kim, Park [38] shows a significant improvement in self-efficacy in nursing students after using a smartphone application for a drug dosage calculation training program. However, there are some considerations to using a smartphone application. Although most calculating applications based on detection algorithms are accurate and useful, some applications were inaccurate [39]. In addition, users in health care professions do not assess the validity of applications regularly [40]. Despite the usefulness, healthcare professionals should utilize them with caution to avoid potential mistakes [41].
In this study, knowledge, accuracy of sepsis assessment, and self-efficacy are interrelated. This result is consistent with Mavis [42]’s study of medical students. The study suggests that knowledge, skill, self-efficacy, and performance are highly related. There are many other studies to support a positive relationship between skill, performance, and self-efficacy [43]. There are not many studies reporting a relationship between knowledge and self-efficacy. Some studies present no relationship between knowledge and self-efficacy [44], while it has been reported that education programs enhance knowledge and self-efficacy together [45]. Although the relationship between knowledge and self-efficacy needs further investigation, it is known that high self-efficacy helps to reduce the gap between theory and practice [46]. Positive self-efficacy induces motivation and eventually changes behavior [19]. For nurses to be more involved in sepsis recognition, an improvement in self-efficacy is required. Because self-efficacy is highly related to knowledge, an increase in knowledge through education is one way to improve the early detection of sepsis.
It is reported that there is no significant difference between traditional lectures, e-learning, and self-study for nurses to acquire knowledge in the short term [47]. Therefore, instead of lectures, this study adopted self-study with an educational booklet for the control group. However, for the purpose of testing the rigorous difference between case-based education and traditional lectures, it is recommended to consider designing research with additional lecture-based education in addition self-study in the future. Another limitations of our study is that the learning process is relatively short. For busy nursing staffs, it can be a strength. However, to increase the effects and embody what they learned, continuous practices may be more effective. In addition, we did not provide high-technology human patient simulators or standard patients in the learning process. A previous study shows that the use of simulators in case-based learning improves patient assessment skill [48]. The use of simulators or standard patients can increase realism. In this perspective, a case-based education applying those components may be considered in the future.
CONCLUSION
In conclusion, case-based learning improved knowledge, accuracy of sepsis assessment, and self-efficacy in sepsis care of nurses working at general wards. The use of a smartphone application is almost equivalently useful to improve sepsis recognition compared to memorization of all criteria. Therefore, case-based learning with the inclusion of smartphone applications is an effective and useful learning method for nurses to detect and manage sepsis patients.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print



